Background
On January 9, 2017, the Centers for Medicare and Medicaid Services (CMS) gave final approval to Washington State for its Medicaid Transformation Project 1115 Waiver for up to $1.125B over five years, for performance-based incentive payments to providers partnering with Washington’s Accountable Communities of Health.
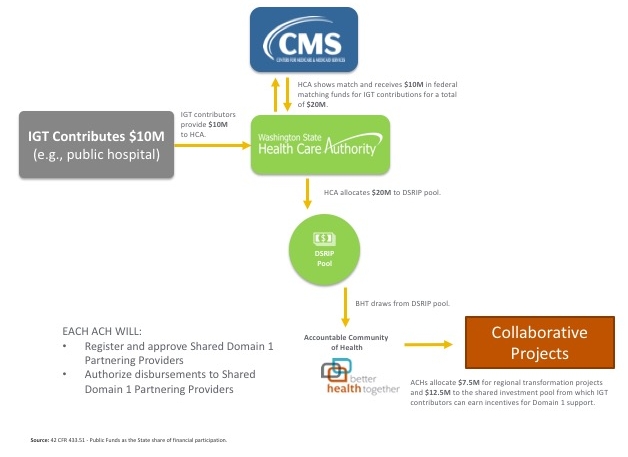
To fund the non-federal share of those payments, Washington State will use a combination of Intergovernmental Transfers (IGTs) from public providers and dollars generated through Designated State Health Programs (DSHPs).
What is Intergovernmental Transfer (IGT)?
A transfer of public funds between governmental entities, such as from a county or a public hospital to the state. The source of funding for each IGT that is proposed by a governmental entity must be reviewed to ensure that it meets state and federal requirements for permissible transfers.
IGT FACTS
- IGT is one of two CMS approved funding sources for the Delivery System Reform Incentive Payment (DSRIP) Program, the other being DSHPs.
- IGT contributors can participate in each of the Accountable Community of Health (ACH) regions and earn incentives as a partnering provider.
- Must comply with the Special Terms and Conditions (STCs) and the approved IGT Protocol
Who can be an IGT contributor?
Essentially, IGT contributors are governmental entities. Our IGT protocol references intergovernmental transfers “from public hospitals, other local government or tribal funds”. The HCA has prioritized governmental entities delivering and/or support health care reform efforts.
Who is responsible for obtaining IGT contributors?
The HCA is responsible for managing IGT contributor relationships including handling the contractual requirements to operationalize the IGT financing mechanism. This includes identifying and securing necessary agreements with IGT contributors in order to establish the mechanism whereby contributions are made. Similarly, it is HCA’s responsibility to claim federal funds, whether based on DSHP or IGT. ACHs are not required to find IGT contributors.
Who are the currently identified IGT contributors?
University of Washington (in association with UW Medicine) and the Association of Washington Public Hospital Districts (initially Evergreen Medical Center and Valley Medical Center) have offered to participate as IGT contributors. Other public hospitals or government entities with the ability and interest to contribute are certainly welcome. It should be noted that IGT funding supports the DSRIP program across ACHs. BHT is committed to exploring expanding the list of IGT contributors to include potential partners in the Eastern Washington.
What are the terms and mechanisms for IGT contribution?
Twice per year HCA will invoice the IGT contributor(s). IGT contributions will be processed through the Financial Executor and deposited to ACH accounts for subsequent release as incentive payments. These contributions will be invoiced only aftter Independent Assessor review, recommendation of incentives, and ACH approval of earned DSRIP payments.
What does this mean for the BHT ACH?
- BHT’s approval of the IGT Strategy funds $46.5M in Shared Domain 1 investments over the five years.
- If one or more ACHs select to not participate in the Shared Domain 1 Investments this will reduce the total available funding available for ACH project incentives both for shared investment and locally controlled project funds.
What are the benefits of IGT financing?
- IGT contributors, like other provider partners, must have an opportunity to earn incentives.
- IGT contributors are well-positioned to provide Domain 1 services across all nine ACHs.
- Incentives are intended to recognize and encourage provider activity that advances the ACH’s delivery system reform goals.
What are Shared Domain 1 Investments?
A term representing pooled incentive funds for specific (to be defined) Domain 1 services from designated providers across all nine regions.
Shared Domain 1 Investments FACTS
- These neither preclude nor replace other ACH allocations for Domain 1.
- These are the incentives to be earned by IGT contributors.
- These incentive funds support the use of IGTs as a funding mechanism for DSRIP.
- ACHs must still approve incentive payments made this pool.
- Payments from pool will be triggered once ACHs determine when a Shared Domain 1 Partnering Provider has met their deliverables statewide.
How may incentive payments be earned by IGT contributors?
As authorized by the ACHs, IGT contributors will (when registered as partnering providers) be given an opportunity to receive DSRIP incentives by supporting Shared Domain 1 services (value-based payment, workforce, population health management). Incentives are intended to recognize and encourage provider activity that advances the ACH’s delivery system reform goals. Incentive payments to those partners providing Domain 1 support services are, like all DSRIP payments, governed by our CMS approved protocols. Those protocols do not distinguish between providers of Domain 1 supports and any other providers with respect to how incentives are allocated by an ACH. Allocation decisions are made by each ACH, and each has the option to participate or not with respect to incentive payments for Shared Domain 1 services.
What are examples of Shared Domain 1 services?
It is anticipated that Shared Domain 1 service descriptions will be developed by the IGT contributors in collaboration with ACHs. For example, the Association of Washington Public Hospital Districts (AWPHD) has agreed to participate as an IGT contribution via contributions by Evergreen Public Hospital District and Valley General Public Hospital District. This gives Evergreen and Valley the opportunity to earn back their contribution plus a 10% return on the investment. An additional portion of the AWPHD’s contribution will be distributed via incentive payments for Public Hospital Districts for At Risk Transformation efforts, and Moving to Value efforts plus investment in AWPHD to support state wide value based payment readiness. As you can see from this example, there is a tangible value to the BHT region for our 6 rural public hospital systems.