As more details on expectations for Medicaid Demonstration Projects trickle down from HCA we are continually refining our project selection process in hopes of making it accessible to all community members interested in participating, while also focused enough to get us ready for the heavy amount of planning we’ll have to do in a very short time. We thank you all for continued feedback throughout this process.
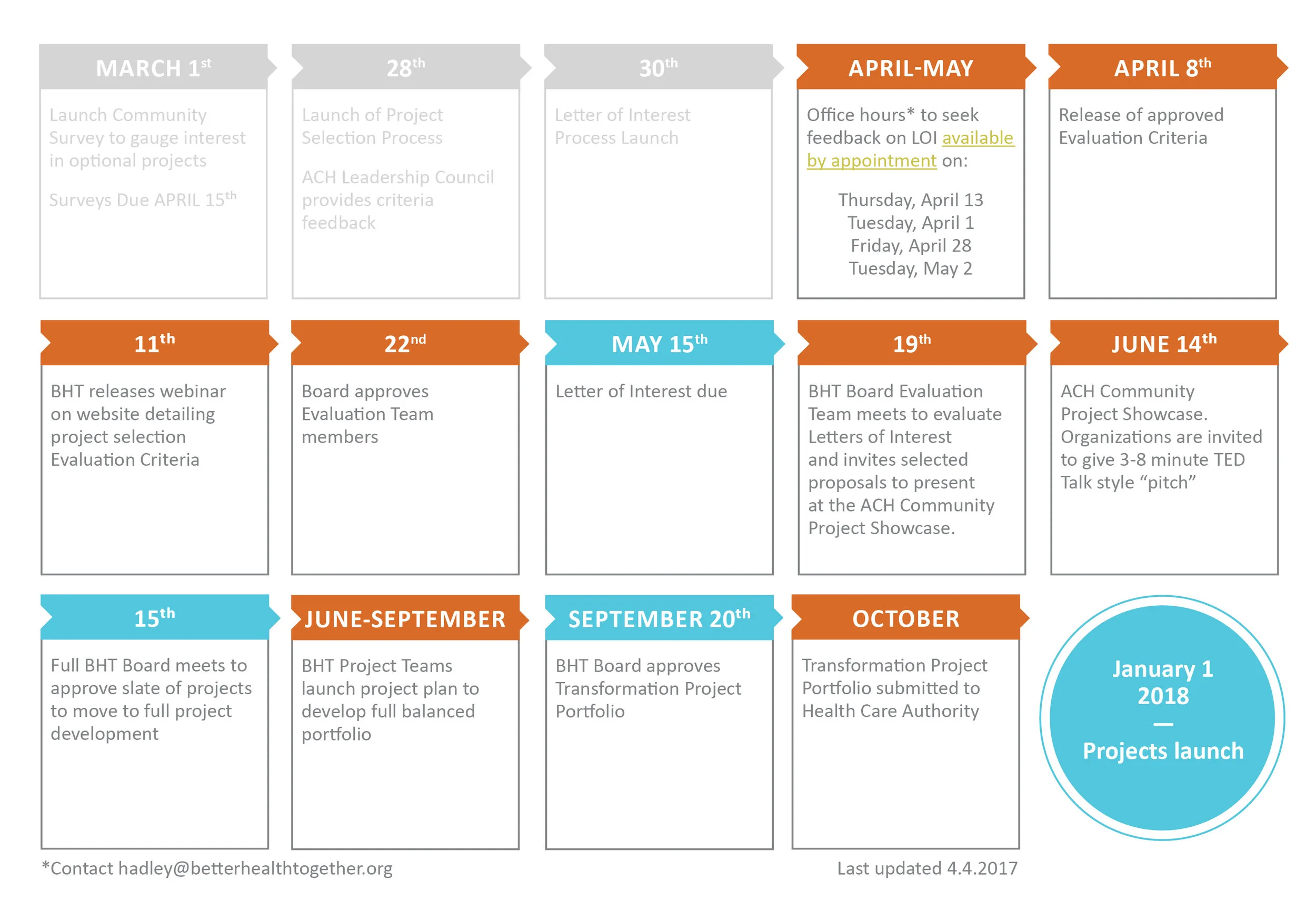
At the March Leadership Council meeting we announced our updated timeline for project selection, which you can view on this one pager. In summary, we are requesting a Letter of Interest from community organizations interested in collaborating on one of the optional Medicaid Demonstration Projects by May 15.
Our Board Evaluation Team will review those letters and invite selected proposals to present at a public Community Project Showcase event, where organizations “pitch” their projects in a short “Shark Tank” styled event. The Evaluation Team and audience members will evaluate project proposals against pre-determined criteria, and from there invite selected projects to continue on to join a planning team and prepare the full application.
Alison’s slides from this presentation can be downloaded here. Though we did not have time to go over them in the meeting, this slide deck includes updated overviews of the Medicaid Transformation Projects from the most recent draft of the toolkit.